Introducing FIRSTmed-ADLX Model: As a New Learner Experience
LX Model in the Medical Context, Public Health and Wellness
Education Intervention – the Case of the IMC Wellness Office in KSA
Mohamed Bahgat1a
Alaa Nazal1b
Ashraf Elsafty2a
Ahmed Seddek2b & Asmaa Elkharoby3
1a Senior Researcher, CEO, SeGa Group, United States. E-mail: mbahgat@segagroup.net
1b Senior Researcher, MD, Executive Director of Academic Affairs & Research Center, IMC, KSA. E-mail:
anazal@imc.med.sa
2a Adjunct Assistant Professor, ESLSCA University, Egypt. E-mail: ashraf.elsafty@eslsca.edu.eg;
ashraf@ashrafelsafty.com
2b Researcher, MBA, Ashraf Elsafty Consulting, Egypt. E-mail: ahmed.seddek@ashrafelsafty.com
3 Project Manager, SeGa Group, United States. E-mail: asmaaelkharoby@gmail.com
Correspondence: Ashraf Elsafty, Adjunct Assistant Professor, ESLSCA University, Egypt. ORCID ID:
https://orcid.org/my-orcid?orcid=0000-0002-9377-7286. E-mail: ashraf.elsafty@eslsca.edu.eg;
ashraf@ashrafelsafty.com
Received: January 8, 2025 Accepted: February 10, 2025 Online Published: February 14, 2025
doi:10.5430/ijhe.v14n1p23 URL: https://doi.org/10.5430/ijhe.v14n1p23
Abstract
The field of health and wellness education in the public health presents unique challenges due to the need for
effective frameworks that can help educators and healthcare providers facilitate the transfer of wellness concepts to
clients for behavior modification and transformation for better health outcomes (Solhi et.al, 2020; Olsen, 2010). In
response to this need, the FIRSTmed-ADLX (Focusing – Interacting – Reviewing – Sequencing – Transforming)
(Active Deep learner experience) was developed as medical education, public health, and wellness sub-context of the
successful FIRST-ADLX framework (Bahgat et al. 2018), This paper explores the compatibility and effectiveness of
the model for public health and wellness education. The study adopts an exploratory mixed research method that
combines qualitative by the template analysis technique using MAXQDA and quantitative for descriptive analysis
using MS Excel.
Findings include the unprecedented paradigm transformation expressed by healthcare providers and medical
educators in their understanding of education and learning principles. The study revealed that participants’ deep
engagement and motivation, coupled with their perception of themselves as learners, greatly assisted them in
enhancing their design and facilitation capabilities by applying the domains and principles of the model. Wellness
clients exhibited notable transformations in their learning experiences and personal behaviors, particularly in
adopting healthier lifestyles and embracing wellness practices.
Furthermore, the analysis has brought to light the notable impact of FIRSTmed-ADLX on the working culture within
the IMC’s (International Medical Center) wellness office results. This encompasses processes, internal language, and
behavioral shifts, underscoring the substantial impact of the model.
Keywords: FIRSTmed-ADLX, learner experience, public health education, wellness education, active deep learning,
impact map
1. Introduction
The field of public health is currently facing several challenges. One significant challenge is the need for healthcare
systems and providers to adapt to the changing causes of diseases and deaths. According to WHO (World Health
Organization), a considerable percentage of deaths in developing countries are attributed to unhealthy lifestyles, and
this number is projected to increase to 70% by 2030 (Home, 2023). Additionally, there has been a shift in the nature
of diseases, with a rise in chronic conditions that are prevalent in society. This shift puts additional strain on the
healthcare system, as it requires a different approach compared to acute or contagious diseases. Dealing with these chronic diseases using conventional clinical methods poses its own set of challenges (Solhi et al., 2020). Furthermore,
the cost of providing healthcare to patients has been on the rise, which presents further difficulties in addressing
these diseases effectively. The increasing costs make it more challenging for healthcare systems and providers to
allocate resources efficiently and deliver adequate care to those in need. (Solhi et.al, 2020).
To achieve health equity and improve population health outcomes while reducing healthcare costs, the healthcare
system requires new interventions. Various interventions have been introduced to address unhealthy lifestyles and
promote behaviors associated with a health-promoting lifestyle. These interventions include frameworks such as
health promotion, health coaching, patient education programs, and self-management programs. These programs aim
to enhance health knowledge and health literacy among clients (Solhi et.al, 2020).
The primary expected outcome for individuals participating in these programs is an enhancement in their quality of
life. Alongside this, patient empowerment, self-efficacy, and self-management are considered crucial intermediate
outcomes. However, it has been challenging to define, measure, and accurately report on these factors in terms of
their impact on patients’ lives (Osborne,2007). Implementing these interventions necessitates healthcare providers
and educators to possess specific attitudes, skills, and knowledge. They need to be capable of designing and
facilitating public health and wellness educational programs for their clients. Training healthcare providers to design
and facilitate health education interventions through learning journeys is essential. The impact of these interventions
is not obvious in the current state as these frameworks are not holistic or comprehensive as they shall be combined to
help healthcare providers and educators to competent designers and facilitators of health and wellness concepts
(Olsen, 2010).
On the other hand, Bahgat et al. (2018) introduced a novel framework for enhancing the learner experience called
FIRST- ADLX framework. where SeGa Group has coined the term ADLX which combines active learning, and deep
learning with experience. FIRST-ADLX is considered a comprehensive framework that draws upon various models
and theories, including experiential learning as developed by Kolb and John Dewey, cooperative learning by Kagan,
facilitation skills by Carl Rogers, Roy’s 6Ds for learning transfer, and principles of positive psychology. Additionally,
group coaching is adopted as a means of promoting deep transformation. By combining insights from multiple fields
such as experience economy by Pine and Gilmore.
FIRST-ADLX framework aims to provide a holistic approach to learning that encourages sustainable positive and
transformational impact in individuals. FIRST-ADLX framework is a comprehensive, research-based framework that
promotes Active Deep Learner experience and inspires a positive transformation in the mindset, skillset, and
performance of the educators. It is built on previous learning theories that have been studied and tracked by the
FIRST-ADLX Framework and introduced this newly different paradigm of ADLX. Each of these learning theories
has its strengths and weaknesses, and not one theory is perfect. FIRST-ADLX framework draws on the strengths of
each of these theories, and it provides a comprehensive framework for designing and facilitating Active deep learner
experience (Bahgat, 2023, P. 25). After conducting several projects with various clients in diverse geographical areas
and contexts, SeGa Group has concluded that FIRST-ADLX framework is both feasible and adaptable for
implementation across different contexts, including education context, medical context, and organizational context.
SeGa Group has leveraged this framework to develop its products and projects, represented by the SeGa Context
Map, which caters to specific target fields and clients. Whether utilizing the FIRSTedu-ADLX model,
FIRSTorg-ADLX model, or FIRSTmed-ADLX model, SeGa’s products can be utilized to cover the entire journey or
select specific products based on specific requirements LXF (Learner experience Facilitator), LXD (Learner
experience Designer), LXC (Learner experience Coach). Figure 1 illustrates SeGa’s Context Map, which has been
designed in alignment with the FIRST-ADLX framework.
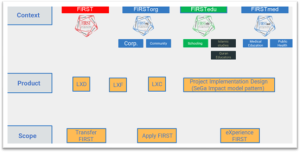
Figure 1. SeGa Context Map (SeGa, 2023)
1.1 FIRSTmed-ADLX Model Intervention in Public Health & Wellness Education
One of the areas where FIRST-ADLX framework has been particularly successful is in medical education and public health and wellness education. To this end, FIRSTmed-ADLX model has been developed to specifically address the unique needs and challenges of medical education and public health and wellness. By tailoring the framework to the specific requirements of medical education and public health and wellness, FIRSTmed-ADLX model can help educators apply in designing and facilitating more engaging and impactful learner experiences either for medical or public health clients.
The AAMC (Association of American Medical Colleges) published a discussion paper titled “How Medical Education is Changing” which highlighted the three phases of medical education as follows: medical school UME (Undergraduate Medical Education) is the first phase of medical education, and it typically includes four years of undergraduate study. During this time, students take courses in the basic sciences, such as anatomy, physiology, biochemistry, and pharmacology. Residency training GME (Graduate Medical Education) is the second phase in medical education where graduates seek a medical license and/or board certification. It is typically designed as clinical training in hospitals, and its duration varies according to specialty but generally forms three to seven year and could be extended to 11 years according to certification and training requirements. CME (Continuing medical education) is the third phase which is conducted after completing medical school and GME where physicians should maintain their board certification through predefined hours of formal continuous learning and education. (Tomorrow’s Doctors, Tomorrow’s Cures | AAMC, n.d.)
Public health and wellness are distinct fields that are advancing beyond medical education. According to the CDC (Centers for Disease Control and Prevention) Foundation, the definition of public health is “the science of protecting and improving the health of people and their communities. This work is achieved by promoting healthy lifestyles, researching disease and injury prevention, and detecting, preventing, and responding to infectious diseases. Overall, public health is concerned with protecting the health of entire populations” (CDC Works 24/7, 2023).
Based on the information provided, it is evident that there are distinctions between medical education and public health and wellness education. In line with the SeGa Context Map, the FIRSTmed-ADLX model specifically focuses on applying the FIRST-ADLX framework within two distinct sub-contexts: Medical Education and Public Health and Wellness education. This indicates that the FIRSTmed-ADLX model is tailored to cater to the unique requirements and objectives of these two sub contexts, ensuring effective experience transfer and application of the FIRSTmed-ADLX model within the sub context of medical and public health and wellness education.
This study primarily focuses on the context of public health and wellness education and aims to utilize the FIRSTmed-ADLX model to transfer it to health professionals and medical educators in the IMC wellness office and help them to apply the model in designing and facilitating the learning journeys.
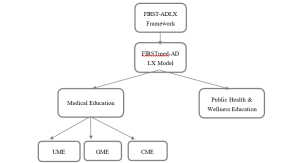
Figure 2. FIRSTmed-ADLX Model Sub context
By collaborating with organizations like IMC through their wellness office and learning project, SeGa Group can facilitate the transfer and application of FIRSTmed-ADLX principles inside clinics (design and facilitating learning) to educators and facilitators, besides can help healthcare providers to develop knowledge skills, and attitude they need to provide an active deep learner experience which empowers them to apply these principles effectively with learners in their journeys.
The primary objective of the project was to transfer the FIRSTmed-ADLX model to health providers within the IMC wellness office and examine the impact of the model on the participating health professionals throughout the whole learning journey, as well as the development of the wellness office team to become educators ( designers LXD, Facilitators LXF) for such health and wellness education intervention to provide learning journeys for the public with lower cost and better health outcomes and overcome public health challenges and chronic diseases ( Cardiovascular diseases, diabetes, obesity, etc..).
Health and wellness are defined not simply as the absence of diseases and their symptoms, but as the constant awareness and effort to choose and practice a lifestyle that holistically achieves wellness. As such the center’s vision has guided the development of public health and wellness educational programs that target both hospital staff and the general public (wellness journeys).
The IMC Functional Medicine & Wellness is one of the IMC departments that treats all chronic illnesses before symptoms appear or after diagnosis by conducting an extensive evaluation of the root causes, identifying imbalances, and promoting a healthy lifestyle based on scientific research. This is accomplished through the collaboration of a team of Physicians, Nutritionists, Psychologists, Health Coaches, and Personal Trainers to initiate the healing process of moving away from illness and towards Wellness.
The wellness office team was eager to design learning journeys for the transfer of wellness education programs to their employees, health care providers inside the hospital, and later on to the entire community so IMC has collaborated with SeGa Group for a wellness education project that aims to achieve the following objectives over an extended period (SeGa Group, 2021).
The project is composed of six primary phases, which are described as follows:
(1) PHASE 1 (Entry to Active Deep Learning / Group Mentoring & Webinars)
At the start of the IMC wellness office project, SeGa group identified significant challenges and obstacles that could impede the desired outcomes and results based on their methodology. These challenges emerged right from the outset and included:
IMC wellness office uses a traditional training approach that heavily relies on a large amount of content and knowledge presentations instead of the full experience of FIRSTmed-ADLX model domains and principles. They have requested a special case of fast-paced learning while integrating the basics, facilitation, and design, and with the rapid production of their programs themselves. Their request was not to go through the same standard SeGa journeys but to only focus on understanding without experiencing and starting to implement directly.
SeGa Group and the IMC wellness office team have reached an agreement regarding their approach, taking into consideration SeGa’s research findings on the learner’s experience and the factors that influence it. It has been emphasized that SeGa does not make specific commitments or promises regarding achieving certain results or impacts within a specific timeframe. Instead, SeGa Group will provide ongoing support by integrating relevant concepts and projects that the IMC wellness office team can begin applying during the mentoring process.
(2) PHASES 2 / 3 (Individual Personalized Journey)
The learners started designing their journeys, and after several meetings, they requested to have mentoring meetings about it. As predicted, several design gaps could only be filled by experiencing an integrated interactive learning journey (SeGa Group, 2021).
During this phase, a customized personalized journey is designed especially for the participants. It comes in two primary categories: Individualized consultations for the three selected learning journeys, “Meaning of life, Gut healing, and Physical wellness” and Group meetings to discuss the center’s holistic map, which includes disclaimer, design, content, persona, and learning outcomes.
(4) PHASE 4: LXF (Learner Experience Facilitator Journey)
When the learners realized that learning through experience is entirely different from being lectured, they accordingly asked to participate in a fully experiential journey, where everything that had been previously exposed to is repeated but with an interactive system within a carefully thought-out framework that takes the learner into account in all its aspects (learner-centric approach).
The main focus of the journey was to enable learners to live an Active Deep Learner experience and practice facilitating an Active Deep Learner experience using the FIRSTmed-ADLX model. This has been done by developing attitudes, skills, and knowledge.
(5) PHASE 5: LXD (Learner Experience Designer Journey)
After experiencing the FIRST-ADLX Facilitator Journey, the learners demanded to attend the FIRSTmed-ADLX Designer Journey to become qualified as a practitioner designer. The approaches used in this journey were Designer Mindsets, FIRSTmed-ADLX Design Maps, and FIRSTmed-ADLX Designer Actions (SeGa Group, 2021).
In addition, several tools and platforms are being used at this stage, including the ID course, co-design mission using Miro, and Session Lab.
(6) PHASE 6: Designer Certificate Track
A certification track with two phases was provided to the participants: the mentoring phase, when each participant designs his pilot learning journey and receives feedback from the mentoring team of Sega Group, Additionally, during the assessment phase, the participant’s performance, Knowledge, and skill are assessed to evaluate the extent of his understanding and application of design mindsets, design map & FIRSTmed-ADLX framework principles and domains.
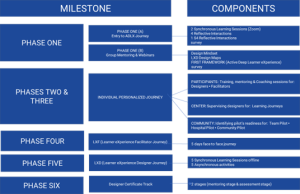
Figure 3. IMC wellness office project phase (2023)
2. Literature Review
2.1 Public Health and Wellness Education
The initial and most well-known perspective on health promotion defines it as “the art and science of assisting individuals in making lifestyle changes to achieve optimal health.” This approach is based on the belief that individuals have significant control over their personal decisions and behaviors related to diet, exercise, and other lifestyle factors and that these changes can greatly impact health outcomes. This viewpoint emerged in response to various factors, including dissatisfaction with the limitations of traditional medicine, efforts to manage healthcare costs, and a societal emphasis on self-help and individual responsibility for health (Minkler,1989).
In this broad and interdisciplinary perspective, the health educator can fulfill specific roles that contribute to advancing the goals of an open society. Their skills and competencies can be utilized to create social and health conditions rooted in health promotion, enabling individuals worldwide to attain optimal health. Ronald Labonte, a Canadian health educator, emphasizes the ultimate challenge for health educators is to work towards establishing a state of health for all individuals by shaping societal conditions that prioritize health promotion (Minkler,1989).
Solhi et al. (2020) findings suggest that educational interventions in health promotion are effective in improving and encouraging health-related behaviors and lifestyle, including various dimensions. Consequently, health education encompasses lifestyle modifications, behavior changes, environmental adjustments, and nutritional aspects. Furthermore, Health coaching is a recommended intervention to assist individuals in achieving behavior change and better health outcomes. The health coaching approach focuses on the patient’s needs, with coaches offering education, feedback, and support to boost self-awareness, motivation, accountability, and self-efficacy. Patients, being experts in their life situations, play a significant role in guiding the learning process and implementing changes. Despite the growing availability of health coaching programs across different settings, many healthcare professionals remain unaware of this beneficial intervention (Olsen,2010). The same concern regarding patient education and self-management programs that gain international interest are still suffering from measuring the impact and transformation of these programs on lifestyle (Osborne, 2007).
Freudenberg’s principles, which form the foundation of health education for social change, offer a significant framework for acting. These principles emphasize the acknowledgment of social and economic factors that influence health and illness. They highlight the necessity of collective action and mutual support, emphasizing the integration of education, service, and political engagement. Additionally, these principles prioritize people and their immediate needs as central to the process of promoting health. Overall, Freudenberg’s principles provide a timely and essential guide for health educators to drive meaningful change (Minkler,1989).
In Alberti’s (2023) work, Frieden’s Health Impact Pyramid has been reimagined as a Population Health Impact Pyramid for Health Care. This reimagining aims to highlight how the field of medicine can contribute to the health of populations through specific actions and collaborations, going beyond individual patient care. The integration of health care into this model provides a framework for medical care organizations to act and make an impact on community, national, and global health. The first tier of the pyramid focuses on health profession education, emphasizing the importance of incorporating population health principles into the curricula for physician learners. While such educational activities may not directly translate to measurable population health outcomes, they play a crucial role in preparing future physicians to contribute to population health improvement efforts. However, there is a need for clear and widely accepted guidelines on the knowledge, skills, and attitudes that all medical professionals should possess to promote population health. Additionally, there is a shortage of faculty with advanced knowledge and skills to effectively teach these essential components. Calls have been made for academic medicine to develop a career track for “physician-public health practitioners” to address these gaps in medical education.
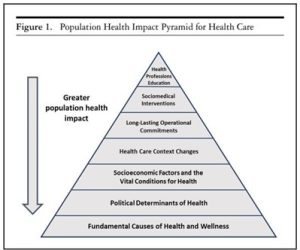
Figure 1. Population health impact pyramid for healthcare (Alberti’s (2023)
2.2 Learning Theories and Frameworks
Transformative learning is a deep shift in perspective during which habits of mind become more open, more permeable, and better justified (Cranton, 2006; Mezirow, 2000). According to Mezirow (1978), the process centers on critical reflection and critical self-reflection, but other theorists (Dirkx, 2001) place imagination, intuition, and emotion at the heart of transformation (Mezirow ,1991).
Transformative learning is the process of examining, questioning, validating, and revising our perceptions of the world (Cranton, 1994). It is a theory about change, fundamental and sometimes dramatic change, in how we see ourselves and the world around us (Caffarella & Merriam, 1999).
one of the critiques of transformative learning theory is that it is too focused on cognitive change. Mezirow’s theory emphasizes the importance of critical reflection, which is a process of examining one’s own beliefs and assumptions. However, some critics argue that transformative learning theory does not adequately address the emotional and spiritual dimensions of learning. They argue that transformative learning can be a deeply emotional and spiritual experience and that these dimensions should be given more attention in the theory.
We are currently in the era of learner experience, where the focus goes beyond the curriculum and addresses specific skills during training. It involves designing a comprehensive experiential learning journey for the learner, incorporating their ideas, emotions, and the emotional dimension.
Within this trend, SeGa Group has emerged to develop and refine a new approach known as Active Deep Learner experience. In our approach, it is not sufficient for learning to be merely active, as it would be enjoyable but lacking in impact. Likewise, alone is not enough, as it would result in a dry experience devoid of engagement. We strive for a balance that combines active engagement and profound exploration to achieve meaningful outcomes.
FIRST-ADLX framework is a holistic one; it is based on other models and theories, such as experiential learning by Kolb and Dewey; gamification and game-based learning; facilitative learning, 6Ds model, as well as positive psychology, experience economy, and neuroscience. The theoretical influence for FIRST- ADLX framework has two parts; the primary theoretical influence is the theories and models that influence the framework as a whole, while the secondary theoretical influence represents theories and models that affect some specific domains of the framework. FIRST-ADLX framework includes five main domains and fifteen principles. These principles act together in an integrated format, creating our Active Deep Learner experience approach (Bahgat et al., 2018).
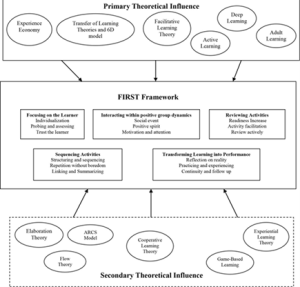
Figure 5. FIRST Framework (Bahgat et al., 2018)
Pine and Gilmore (1998) introduced the concept that experience constitutes a fourth stage in economic offerings, alongside the three traditional stages of economic offerings: commodity offering (dealing with raw materials like coffee beans), goods offering (involving the manufacturing and preparation of coffee beans), and service offering (where restaurants serve coffee). They argued that services, much like commodities, have become commoditized and that creating a distinct and memorable experience is crucial. To achieve this, consumers should actively participate and feel a sensation, requiring highly skilled individuals who can personalize each event according to customer needs.
Graham et.al, (2015) contended that higher education should adapt to the experience economy instead of providing standardized information. This perspective aligns with the idea that making the learner’s experience memorable can enhance the impact of learning. Pine and Gilmore (1998) also suggested that participants in training are more likely to apply their acquired knowledge to real-life practices if the training is enjoyable. In their recent article, Pine and Gilmore (2022) discuss the concept of “Transformations,” which extends the progression model to a fifth level. This level involves companies actively assisting customers in achieving significant changes and prioritizing customer success.
To effectively compete in the domain of transformations, companies must engage in meaningful interactions with customers at various points along their transformation journey. FIRST-ADLX Framework incorporates the principles of experience economy as a foundational theory. Within this framework, the “T” Domain emphasizes the transformation of learning into practical performance. This domain is centered around identifying activities and actions that can be implemented in the training environment to ensure that learners are not only engaged in the learning process but also capable of applying what they’ve learned. Additionally, it addresses the crucial aspect of follow-up and mentoring that may occur after the initial training. To achieve these goals, the framework relies on three key principles “Reflection on Reality”, “Practicing and Experiencing”, and “Continuity and Follow-Up”.
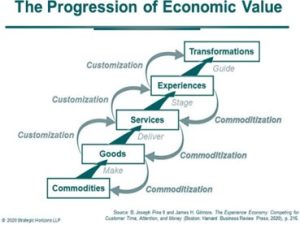
Figure 6. experience economy theory (pine and Gilmore, 1998)
SeGa group has implemented Impact Map Version 2 to evaluate the impact of the FIRST-ADLX framework and its contextual models such as FIRSTmed-ADLX on the learning ecosystem. Another model used to assess the effectiveness of training and learning activities is the Kirkpatrick Model (1976). This model evaluates training techniques, both formal and informal, and ranks them according to four levels of standards: (Level 1: Reaction) The reaction level is the most basic level of evaluation, it measures how participants reacted to the training. (Level 2 Learning) The learning level measures what participants learned during the training. (Level 3: Behavior) The behavior level measures whether participants changed their behavior because of the training. (Level 4: Results) The results level measures the impact of the training on the organization. However, it is important to note that the Kirkpatrick Model is not perfect. It does not measure all aspects of training effectiveness, and it can be difficult to obtain accurate data at the higher levels.
Despite its limitations, the Kirkpatrick Model is a valuable tool for evaluating training programs. It can help organizations to improve their training programs and to make sure that they are getting a return on their investment in training.
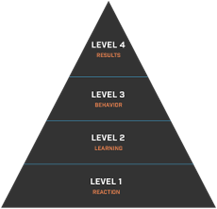
Figure 7. Kirkpatrick’s Model (Kirkpatrick,1994)
Kirkpatrick, in his work (2015), has not only maintained the original Kirkpatrick Model but has also introduced new elements to guide organizations aiming to operationalize the model effectively. This guidance is particularly pertinent at levels 3 and 4, which offer the necessary data for measuring training effectiveness in terms of job performance and organization results. These aspects are frequently overlooked by the majority of training programs, which tend to concentrate solely on measuring and attaining levels 1 and 2.
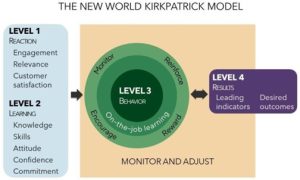
Figure 8. The New World Kirkpatrick Model (2015)
Bahgat et al. (2017) used the Kirkpatrick Model to evaluate the effectiveness of the FIRST-ADLX framework in Malaysia through a project named “ROOTS”., particularly at levels 1 and 2. The results showed that all teachers who participated in the “ROOTS” program reported a significant positive change in their attitudes towards three domains: the importance of the teacher’s role, their appreciation of the FIRST-ADLX framework, and their willingness to apply it. Participants appreciated how the FIRST-ADLX framework would help them to make the learning experience of their students more impactful, sustainable, and life-changing. Furthermore, the study reveals that the FIRST-ADLX framework is an effective tool for improving teacher attitudes and practices. The framework can help teachers to become more effective educators and to create a more engaging and effective learning environment for their students.
Bahgat et al. (2020) have qualitatively and quantitatively validated the implementation of the FIRST-ADLX framework in TPD (Teachers’ Professional Development) in the “ROOTS” program. The objective of the project was to qualify 107 teachers to become FIRST-ADLX facilitators.
Bahgat et al. (2020) have created an impact map version 1 to assess the effectiveness of the FIRST ADLX framework. This map comprises six main themes and 20 sub-codes, which were derived from a qualitative analysis of feedback provided by users regarding the impact of the FIRST-ADLX framework as shown in Figure 9.
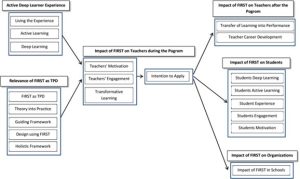
Figure 9. FIRST-ADLX Impact Map version 1 (Bahgat et al.2020)
To ensure the successful application of FIRST-ADLX Framework for achieving the intended impact on various aspects of the learning ecosystem, SeGa has created a FIRST-ADLX Impact Map version 2 based on Kirkpatrick Model. The map illustrates all the components and aspects that FIRST-ADLX framework has an influence on, which are directed by SeGa’s various products. The Impact Map has been designed to align with the Impact Map Version 1 proposed by Bahgat et al. (2020). This alignment allows for clear visualization and connection between all the components of the FIRST-ADLX framework and their impact sphere and outreach.
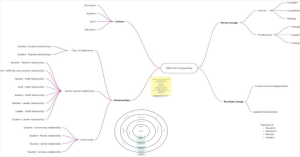
Figure 10. FIRST-ADLX Impact Map-V2 (2023)
2.3 Bridging the Gap
In conclusion, the current state of public health and wellness education lacks a definitive framework or specialized programs that effectively design and facilitate learning in this field. Additionally, existing programs in public health and wellness education often fail to bring transformation or learner experience at both the individual (healthcare providers) and community levels. Therefore, there is a significant demand for a comprehensive learning framework that can elevate public health and wellness education to a new level. This need became evident through the implementation of FIRSTmed-ADLX in the IMC wellness office, where healthcare professionals acquired the requisite mindset, skillset, and toolset to effectively design and facilitate public health and wellness education for their clients. This resulted in a notable paradigm shift at the personal level of healthcare professionals and educators and within the IMC wellness office.
3. Methodology
This study adopts an exploratory mixed research method that combines both qualitative and quantitative data collection techniques. The aim is to enhance the trustworthiness of research findings and the validity of inferences drawn (Bryman, 2006; Saunders et al., 2009). Qualitative analysis will be performed using the template analysis technique. This involves predefined themes and codes based on the FIRST-ADLX Impact Map while allowing for flexibility in terms of adjustments, such as adding or removing elements, changing scope, and reclassifying themes or codes (King, 2004).This methodology is fashioned by integrating components from the Impact Map V2 (SeGa, 2023), the New World Kirkpatrick Model (Kirkpatrick, 2015), and the FIRST-ADLX Impact Map version 1 (Bahgat et al., 2020). By amalgamating the elements of these three frameworks, a comprehensive map is constructed to convey precise themes and codes. This map serves to provide both concise and in-depth measurements of the impact of FIRST-ADLX and will be customized for FIRSTmed-ADLX. Additionally, quantitative data analysis will be employed, primarily for descriptive analysis using Excel, to validate some of the qualitative findings that correspond to the predefined themes and levels.
3.1 Data Collection Methods
The study involved 20 participants, including healthcare providers and medical educators from the IMC wellness office. Qualitative and Quantitative data were collected from these participants during and after each project phase. Specifically, there were 11 participants in the entry to ADLX phase, 8 participants in the LXF phase qualified from phase one, and 9 participants in the LXD phase qualified from phase two, where the program was designed that in order to progress to the next phase, participants needed to successfully complete the requirements of the previous phase.
Qualitative data were collected using focus groups, mixed surveys (Qualitative and Quantitative), participants’ testimonials written and videos, observations, and participant’s comments on LMS and participant self-reflection. Quantitative data were integrated and embedded within the mixed surveys (Qualitative and Quantitative) and were collected concurrently.
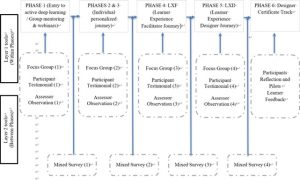
Figure 11. Data Collection Method
3.2 Research Questions
This paper studies the impact of FIRSTmed-ADLX journeys on the members of The IMC wellness office. To achieve this purpose, the following research questions were formed:
Research Question 1: How effective or impactful is the FIRSTmed-ADLX model for public health and wellness education?
Research Question 2: What is the impact of the FIRSTmed-ADLX model on healthcare and medical educators before and after experiencing the model?
Research Question 3: What is the impact of the FIRSTmed-ADLX model on healthcare and medical educators before and after LXF?
Research Question 4: What is the impact of the FIRSTmed-ADLX model on healthcare and medical educators before and after LXD?
Research Question 4: What is the impact of the FIRSTmed-ADLX model on IMC wellness office teams and wellness office units as a whole?
The research questions will try to cover most of the themes that are presented in the impact map.
4. Data Analysis, Results & Discussion
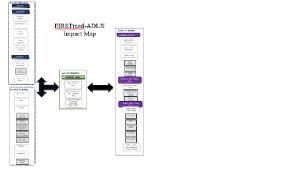
Figure 12. FIRSTmed-ADLX Framework Impact Map
MAXQDA Thematic Analysis was utilized to implement the FIRST-ADLX framework Impact map V3 in the context of the IMC wellness office.
4.1 Level 1: Reaction
4.1.1 Satisfaction
Trainee satisfaction has been defined as the feelings and opinions of trainees on matters or issues during their training (Prystowsky & Bordage, 2001). For instance, their self-confidence, the supervision given by faculty, and societal issues are some issues that trainees will have feelings and opinions on during their training. Moreover, according to Stan et.al, (2020), trainee satisfaction can be driven by the feeling of the success of completion of a task and the feeling of belonging. The quotes from participants regarding satisfaction were as follows:
“The trip was more than amazing I truly learned a lot.” (Participant) “It was a fantastic helpful journey.” (Participant)
“For me, the journey achieved impactful and enjoyable learning that I have always desired in education and training.” (Participant)
“It was an enjoyable, rare, different, and new journey that proved learning is deeper and more beautiful than commonly thought.” (Participant)
The quantitative data have shown that when the participants are asked about their general evaluation of the learning journey in all aspects that all responses are between excellent with almost 85% and very good with 15% as shown in figure 13.
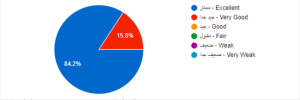
Figure 13. Wellness & Medical Educator satisfaction Descriptive
4.1.2 Engagement
(1) Engagement Statement
Educational researchers have identified three levels of learner engagement: behavioral, emotional, and cognitive (Pintrich & De Groot 1990; Gregory et al. 2013). The quotes from participants regarding engagement were as follows:
“My initial impression is that it’s great that they experienced the atmosphere of offline interactions, and I believe Dr. Mohammed had a comment on that. In the end, we all got a taste of it. Additionally, the participants were highly engaged, and there was even a discussion on how we can recreate this offline experience online.” (Participant)
“The facilitators’ focus on each individual throughout the learning session and spending time with the learners even during break times, not feeling the passage of time due to the role of the facilitator and the variety of activities and interactions.” (Participant response when asked about most positive learning moments)
“The whole journey was active; no boredom the facilitator was brilliant in grabbing the attention and keep me engaged all the days.” (Participant)
(2) Active Learning
Active Learning is defined as “instructional activities involving students in doing things and thinking about what they are doing” (Bonwell & Eison, 1991, p.5). They propose that for the learners to be active learners, they should not only just listen, but they should also write, read, discuss, and solve problems. The quotes from participants regarding active learning were as follows:
“The activities were positive due to their diversity, which enabled me to see the same concept from multiple angles and in different contexts”. (Participant)
“There is hands-on learning and experimentation, making the learning process more effective.” (Participant)
(3) Deep Learning
Biggs and Tang (2011) asserted that a deep approach encourages learners to seek underlying meanings, relate new knowledge to prior experience, and analyze and evaluate the new knowledge. Laird et al. (2005) suggested that when educators use deep learning strategies, learners tend to retain, integrate, and transfer information at higher rates. One of the indicators of deep learning as suggested by Biggs and Tang (2011) is the willingness of the learner to know more information about the topic beyond the curriculum. The quotes from participants regarding deep learning were as follows:
“Now that I am reading the pdf files I hear the voice of Eng Bhagat in my head – with focusing, interacting…. And with every domain, we have the subdomains strongly learned and memorized… the whole journey was fun and entertaining yet at the same time very informative… true Experience of deep learning. Also, I really really liked the water and cup example – I think it is brilliant, very informative yet funny and interactive… loved everything about it, thank you very much.” (Participant)
“It touched some deep miss organized thought about teaching with surrounding, that after the ADLX journey, I am more organized, relaxed and standing on a sold humanitarian way of thinking.” (Participant)
“We came out of the experience with a wonderful understanding and memorization of terms and their meanings to the extent that we now use them automatically.” (Participant)
(4) Living Experience
The learning experience includes every experience they have during the learning journey such as the facilitation method of the educator, curriculum and content, and learning activities (Harvey et al. 1992; Benckendorff et al. 2009). Learning experiences are complex and have different facets; it is in the mind of the individual who has been engaged in the experience emotionally, cognitively, physically, or even spiritually (Pine and Gilmore, 1999; Benckendorff et al. 2009). The quotes from participants regarding living experience were as follows:
“Since the first station at the beginning of the journey until the last station, it left a big and deep impact on myself and the overall experience. The attention to detail, the facilitative style, and the energy present in the group had an unforgettable positive impact.” (Participant)
“The whole journey is positive, enjoyable, and beneficial in all its details.” (Participant) “Every learning day was different and had very unique experience.” (Participant)
“The journey was Inspiring and Motivating.” (Participant)
“It was an enjoyable journey with a lovely group that broadened my thinking from various angles and opened my eyes to different aspects of a new learning experience.” (Participant)
“An unforgettable firsthand experience.” (Participant) “Enjoyable, enthusiastic, and beneficial journey.” (Participant)
“The experience was super pleasant yet informative and transformative.” (Participant)
(5) Motivated for Learning
Motivation refers to learners’ desire and willingness to deploy effort toward and persist in the learning task (Ratey, 2001; Schunk et al. 2008). Many researchers suggested that teachers as adult learners consider motivation as one of the important concepts to a successful TPD (Castañeda, 2016). Moreover, a common problem that faces facilitators is learners’ reticence in the training room which can be mitigated by establishing a safe environment in the training room (Marchand, 2012). The quotes from participants regarding motivation for learning were as follows:
“The enthusiasm that was present from day one continued with me until the end of the journey. It was a distinctive hands-on experience for applying experiential learning through educational interactions and creativity in participation, as well as changing interaction groups according to the exercise. Similarly, the smoothness in the process and repetition was done without boredom.” (Participant)
“They are enthusiastic, and the evidence is that they started dividing the projects, and they have the desire to hear feedback.” (Observer feedback)
The participants were asked about their enthusiasm for the concepts covered in the webinar and their willingness to continue studying them. The results, measured on a Likert scale from zero to five, indicated that all participants agreed with total 100% that they are inclined to continue learning and feel enthusiastic about further studying FIRSTmed-ADLX model domains and principles as shown in figure 14.
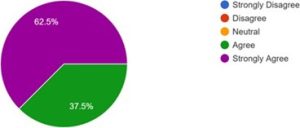
Figure 14. Wellness and Medical Educators Motivation for learning Descriptive.
4.1.3 Relevance
(1) Professional Development
Career Advancement As suggested by (Angadi, 2013; Rose and Reynolds, 2006) teacher professional development programs should be relevant to teachers’ needs. According to Timperley et al. (2007), teachers in the TPD program are more likely to be engaged if they find the program relevant to their professional careers. The quotes from participants regarding professional development g were as follows:
“I got very excited about our physical wellness program; we need to make the pilot alive.” (Participant)
The participants were asked about to which extent the learning journey was effective and relevant to their interest The results, measured on a Likert scale from zero to five, indicated that all the participants agreed that they found the FIRSTmed-ADLX models’ domains and principles is relevant to them as shown in figure 15.
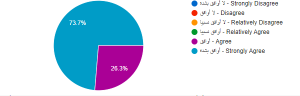
Figure 15. Learning Journey Relevance Descriptive
(2) Theory into Practice
Taking theory into practice is essentially a matter of transfer—applying teaching and learning principles in new situations. New ideas about transfer have implications for both research and practice. The quotes from participants regarding theory into practice were as follows:
“Now, not tomorrow!!! We are on track to empower those who have a significant role in the educational process, starting with learning and then transferring and implementing it across all educational frameworks within the institution.” (Participant)
The participants were asked if the learning concepts covered in the webinar are applicable to their professional practice. The results, measured on a Likert scale from zero to five, indicated that 75% of the participants agreed that they are found the FIRSTmed-ADLX models’ domains and principles can be applied int their professional practices in IMC wellness office.
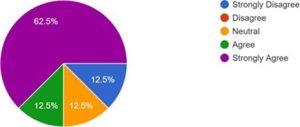
Figure 16. Theory into Practice Descriptive
4.2 Level 2: Learning
4.2.1 Knowledge
Knowledge refers to the extent to which individuals possess specific information, encapsulated by the expression, “I know it.” (Kirkpatrick,2015). The quotes from participants regarding knowledge were as follows:
“We came out of the experience with a wonderful understanding and memorization of the terms and their meanings in such a way that they have become used automatically.” (Participant)
“All the details were inspiring, providing new information that expanded the understanding”. (Participant)
4.2.2 Skill
Skill pertains to the level of proficiency individuals possess in executing a particular action or completing a specific task, as illustrated by the phrase, “I can do it right now.” (Kirkpatrick,2015). The quotes from participants regarding skill were as follows:
“I developed the skill of adapting to new situations, appreciating the diversity and new learning opportunities as well as utilizing new minds and fresh perspectives and not to hold on rigidly to preferred concepts and ideas.” (Participant)
“I am grateful for the skills and enlightening insights I gained from this journey and excited to use them towards creating impactful learning journeys in the future.” (Participant)
4.2.3 Attitude
(1) Guiding Framework
According to the researchers’ analysis of the qualitative data collected from program participants, participants reported that the FIRSTmed-ADLX model offered them clear guidance and direction during their learning and training sessions. The quotes from participants regarding guiding framework were as follows:
“It opened my mind to the idea that it is important to design a journey which the learner benefits from not by knowing more, but by doing more.” (Participant)
(2) Holistic Framework
Holism or holistic education is the educational philosophy consistent with the transformative view. It centers on the principle of interconnectedness and seeks to integrate multiple levels of meaning and experience (Miller 1996). The quotes from participants regarding holistic framework were as follows:
“I anticipate that if the FIRST-ADLX framework is used, there will be a complete revolution in all areas of medical education, as well as in other areas like scientific research and others. This is because the facilitation process in this framework will help lay down clear foundations for assessing the learning, which will be followed by the evaluation of learning processes.” (Participant)
(3) Motivating for Performance
Recently, Duckworth (2016) developed the Grit theory which links the constructs of enthusiasm and persistence to peoples’ potential to effectively reach their goals. Grit indicates the reason some humans succeed in pursuing their goals and the reason some humans fail, which is described as “enthusiasm and persistence for long-run objectives” (Duckworth et al., 2007). The quotes from participants regarding motivation for performance were as follows:
“They are enthusiastic, and the evidence is that they have started dividing the projects and they have the desire to hear feedback.” (Observer feedback)
“In truth, I would like to delve deeper and continue exploring the journey of experiential learning for myself as a learner, so that I can proceed towards designing and facilitating journeys of experiential experiences for learners.” (Participant)
“By now we know the FIRST-ADLX framework very well – we learned so much, all I need to do is free good time to start proper implementation. Implementation needs time, focus and attention to details and I’m so looking forward to delivering a successful program.” (Participant)
(4) Personal Mindset Change
(Habit of Mind) Mindset understood through the worldview perspective focuses on the interaction between the mindset owners and the global/local environments. The mindset here is “a habitual or characteristic mental attitude that determines how people will interpret and respond to situations” (Hyper Dictionary, 2003). People originate their worldview from the unique experiences they have perceived, on their own or through heritage, and then forge their opinions and engage in activities based on their worldview. A worldview describes “a consistent and integral sense of existence and provides a framework for generating, sustaining, and applying knowledge.” (WorldIQ, n.d.) (Fang et al., 2004). The quotes from participants regarding personal mindset change were as follows:
“It’s wonderful in many aspects. We have learned how to perceive things as experiences, not just as content.” (Participant)
“The word ‘school’ and what comes to mind when we hear it? How can one not be concerned with the content or knowledge, but with the experience we went through during the years of schooling?” (Participant)
(5) Professional Mindset Change
For the learning experience to be transformative, educators should introduce adult learners to different perspectives that challenge their frames of reference within a safe environment and mutual trust (Taylor, 2000). This could encourage adult learners to question their held beliefs, feelings, and thoughts which could help them change their attitudes and apply the relevant skills and experiences that they newly acquired (Mezirow, 1994; Curran and Murray, 2008). The quotes from participants regarding professional mindset change were as follows:
“ADLX framework is a transformative experience for me because it created a mindset shift in my understanding of education and it took me from my earlier understanding of an educational system of having you know a lecture within an activity and then where participants are just listeners and just a receiver to you know created a paradigm shift in which the participant is actively and deeply involved in the learning experience for it to become not only knowledge.”(Participant testimonial)
“I will never use the traditional educational approach in the workplace and will instead try to incorporate even a small amount of the fantastic framework.” (Participant)
4.2.4 Confidence
Confidence is delineated as the extent to which training participants believe in their ability to apply the acquired knowledge and skills from training in their professional tasks, as characterized by the phrase, “I think I can do it on the job” (Kirkpatrick,2015). The quotes from participants regarding confidence were as follows:
“I find it easy to apply the concepts.” (Participant) “Everything we learned was applied.” (Participant)
The participants were asked if the learning concepts covered in the webinar will help them to improve their way of working inside the wellness office. The results, measured on a Likert scale from zero to five, indicated that 62.5% of the participants agreed that they are found the FIRSTmed-ADLX models’ domains and principles will help them to improve their professional practices in IMC wellness office as shown in figure17.
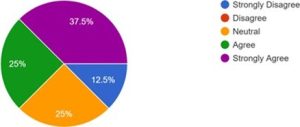
Figure 17. Confidence Descriptive
4.2.5 Commitment
(1) Intention to Action
The extent to which learners have the intention to apply the knowledge and skills garnered from training in their job roles is denoted, it is characterized by the phrase, “I will do it on the job. (Kirkpatrick,2015). The quotes from participants regarding intention-to-action were as follows:
“After discussing the holistic maps, I’ll start applying what I have learned to my project.” (Participant) “I will use everything I learned in my new job.” (Participant)
“I am on my way to designing deeply engaging learning journeys using the FIRST framework. I aim to practice and refine this knowledge and skill to effectively transfer impact and assist individuals in enhancing their well-being in all its dimensions.” (Participant)
“Start to apply some concepts to a real program I am designing.” (Participant) “Start designing training programs.” (Participant)
4.3 Level 3: Behavior
4.3.1 Professional Change
(1) LXF: Change Inside IMC Wellness Office
The healthcare providers reported that the FIRSTmed-ADLX model provided a comprehensive approach to learning that covered not only medical knowledge but also interpersonal skills, communication, teamwork, and personal development. They also highlighted how the framework encouraged active learning, critical thinking, and problem-solving, and helped learners to apply their learning in real-life situations. The quotes from participants regarding professional change were as follows:
“I had never experienced the principles and domains of the FIRST-med ADLX model before, and I had never experienced it in multiple roles, including that of a learner who encounters the FIRST-med ADLX model and is influenced by the learner’s deep active experience itself, as well as how he designed and facilitated programs that, God willing, convey this hoped-for and sustainable impact.” (Participant)
“Getting to know colleagues at work well, which might not have been possible in other contexts. Recognizing the human aspect in learning – even if it was mentioned humorously: considering difficulties in all their dimensions and evaluating learning.” (Participant)
“The inclusivity of humans in the educational process is very important and has great depth in facilitating.” (Participant).
Another measure of the impact of the FIRSTmed-ADLX model on the IMC wellness office team’s satisfaction and loyalty after facilitation journey is the Net Promoter Score (NPS) introduced by (Fred Reichheld, 2011). NPS is calculated by subtracting the percentage of promoters from the percentage of detractors. Based on the data collected, the NPS for the model is 73.6%, indicating exceptional satisfaction and outstanding loyalty and impact on the learners after experiencing the LXF.
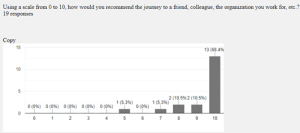
Figure 18. LXF NPS
(2) LXD: Change Inside IMC Wellness Office
Design using the FIRSTmed-ADLX model comes with creating the conditions and utilizing the available resources to provide facilitators with the activities, content, and session flow that help them motivate their learners to learn. One healthcare provider described this as:
“After having enough time to practice and getting familiar with all the design tools, maps, and background knowledge (which was not easy for me as a naïve person in the field of learning and coaching) I realized the importance of having a methodology to design the learning process; to design learning process in contrast with my previous paradigm i.e.: providing knowledge.” (Participant)
“The piloting mindset helped me to “fail early”, which was expected to happen due to the philosophical nature of the topic. The structure of the design thinking gave me clarity about the learner’s needs: more/less content, energizers, cognitive and emotional status… etc. as well as the designer’s needs: inspiration, clarity of the outcomes, empathy, deeper understanding of the persona… etc.” (Participant)
“As a designer I experienced shuffles and changes in role. This taught me flexibility and maturity and not to be attached to the journey emotionally. It also taught me acceptance and how to adapt to new situations. Most importantly it taught me the importance of documentation and following a methodology and following the process, and to simply trust the process.” (Participant)
“The challenges I’ve faced in the past have had a significant impact on how mature I’ve become as a designer because they’ve given me the mindsets and design tools that have helped me move between and around more easily while designing, viewing Design Maps as a free space that supports rather than limits design decisions. Incorporate (FIRST Principles & Domains) into the design and the content of the facilitator’s instructions.” (participant)
“After experiencing the designer’s journey, during my subsequent experiences as a designer, I felt more comfortable experimenting with design mindsets and tools that made it simpler for me to move in and around more fluidly, viewing maps as free spaces that supported, rather than constrained the design. Take part in helping the team finish a variety of design jobs and activities in a timely manner and with appropriate effort. Release a prototype, give it a try, and then deepen and refine it. Always wear different hats.” (Participant)
Another measure of the impact of the FIRSTmed-ADLX model on the IMC wellness office team’s satisfaction and loyalty after facilitation journey is the Net Promoter Score (NPS) introduced (Fred Reichheld, 2011). NPS is calculated by subtracting the percentage of promoters from the percentage of detractors. Based on the data collected, the NPS for the model is 80%, indicating exceptional satisfaction and outstanding loyalty and impact on the learner in IMC wellness office after experiencing LXD.
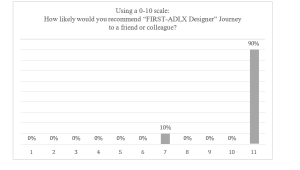
Figure 19. LXD NPS
(3) Relationships inside IMC
The quotes from participants regarding relationships were as follows:
“Visual representation of the efforts (portfolio, piloting, and prototypes) is an excellent way to communicate with the managers and colleagues.” (Participant)
“I experienced significant growth in collaboration with my colleagues. This activity appealed to me because if it resonated with me, I knew I would enjoy it. Immediately, I reached out to my peers and discussed the activity with them, embracing a collaborative mindset.” (Participant)
“I sought the help of my colleagues who were also undergoing the design experience in bridging the gap and selecting the content.” (Participant)
4.4 Level 4: Results
4.4.1 Leading Indicators
The participants were required to design and facilitate a pilot project of educational programs aimed at educating wellness clients on how to lead a healthy lifestyle. They were also responsible for collecting feedback from the clients regarding their wellness journey.
(1) Learner (Wellness Client) Satisfaction
As indicated by the clients’ reflections, the feedback was as follows:
“Positive and happy” (Wellness Client)
“Wonderful, fruitful, and the team is very cooperative’ (Wellness Client)
(2) Learner (Wellness Client) Engagement
As indicated by the clients’ reflections, the feedback was as follows:
(3) Learner (Wellness Client) ADLX Perception
Active Learning “An extraordinary journey, breaking the routine, enlightening, engaging, and encouraging experience” (Wellness Client)
Deep Learning “Many thanks to all those involved in the wellness journey. You have creatively and entertainingly introduced a new perspective on wellness, offering valuable and distinctive insights” (Wellness Client)
Living the experience “An enriching and enjoyable experience” (Wellness Client)
“An excellent and beneficial experience” (Wellness Client)
4.4.2 Results on the Organization
(1) IMC Wellness Office Culture
Organizational Behavior Change IMC Team members as physicians or healthcare providers are affected by the journey not only as educators but also as health providers with clients. So, these practices changed even in the clinic with the clients. Quotes from participants regarding organizational behavior change were as follow:
“Even performance in the clinic is significantly affected by experiencing the journey; this is the epitome of a learning experience.” (Participant)
“Since our organization attended, I noticed a significant difference in each employee’s passion, integration, transformation, and effective team spirit, which I would like to generalize to the level of many departments.” (Participant)
“I experienced a significant improvement in collaboration with my colleagues. I liked this activity because if it’s done with me, I will immediately call my colleagues and discuss it with them collaborative mindset.” (Participant)
Process / Language within IMC Wellness Office have undergone significant changes, leading to a shift in team collaboration and interaction patterns.
“I got very excited about our physical wellness program we need to make the pilot alive.” (Participant) “Division name should be Learner rrrrrrrrrr experience.” (Participant)
“There has been significant progress because I used to get really annoyed when someone told me that a certain activity wasn’t suitable. I used to cling to my own opinion. But now, my way of thinking has changed to a ‘growth mindset,’ and this shared language has become common throughout the IMC level.” (Participant)
“I experienced significant development because I used to get very upset when someone told me that this activity was not suitable, and I used to stick to my opinion. But now, my way of thinking has changed to a “growth mindset,” and this common language has become part of IMC wellness office.” (Participant)
4.4.3 Learner (Wellness Client) Impact
(1) Learner (Wellness Client) Learning
“Reflections on the Pilot of one of the participants “FIRST-ADLX I see more of creativity and Focusing on the learnerrrrrrr” (Wellness Client)
Knowledge “I learned how to live my life in health and wellness” (Wellness Client) “Very informative and impactful” (Wellness Client)
Skill “I enjoyed and benefited a lot, and I gained self-awareness.” (Wellness Client)
Attitude “A fun and wonderful journey that clarified many aspects in our lives that we tend to overlook” (Wellness Client)
Confidence “Beautiful and enriching, every time I get to know myself more and know more” (Wellness Client) Commitment “Adopting a healthier lifestyle is the fastest and easiest way to change my mental state” (Wellness Client)
(2) Learner (Wellness Client) Change Character
1) Behavioral Personal Change
The IMC wellness office presented a workshop, and they asked the facilitator to practice some FIRST-ADLX concepts without experiencing it and below are the comments on this workshop.
“The workshop” Your Well-being in Ramadan: The Month of Detox and Beautification” was not designed within the FIRST framework, but it greatly influenced us. The meeting was beautiful and attended by 100 people with the aim of raising awareness and promoting the message. It was a new experience for Dr. Walid, who actively engaged in it for the first time, and he was pleased with it. We requested him to actively participate. However, this is just a measurement in theory. We are successful; I do not expect to measure the degree of people’s paradigm shift, but based on the interaction, it seems that some of them benefited, and the overall atmosphere was very positive indeed.
“Self-awareness of my well-being, entering the wellness journey with gentleness, the joy of participation, listening to others’ experiences, and making decisions on the path of assistance” (Wellness Client)
“The program is very profound; it has changed my perspective on life” (my life) (Wellness Client) “A new vision for self-wellness” (Wellness Client)
“A really close look on yourself” (Wellness Client)
During the analysis, some interesting relationships between components of the impact map have emerged, based on the healthcare providers’ and medical educators’ perspectives as shown in Figure 12. For instance, when healthcare providers express an intention to apply FIRSTmed-ADLX in their work, they tend to feel enthusiastic about their career development journey with FIRSTmed-ADLX. On the other hand, when a participant experiences the learning journey as a learner, they become deeply engaged emotionally, cognitively, and behaviorally. These relationships can enhance the impact of FIRSTmed-ADLX on both the overall program and the corresponding themes. By acknowledging and leveraging these relationships, facilitators or designers of FIRSTmed-ADLX can further enhance the effectiveness of the program and its impact on learners’ development.

Figure 20. Relation between codes (MAXQDA)
5. List of Abbreviations
Table 1. List of Abbreviations
| Abbreviation | Meaning |
| FIRST | Focusing – Interacting – Reviewing – Sequencing – Transforming |
| ADLX | Active Deep Learner experience |
| IMC | International Medical Center |
| WHO | World Health Organization |
| LXF | Learner experience Facilitator |
| LXD | Learner experience Designer |
| LXC | Learner experience Coach |
| AAMC | Association of American Medical Colleges |
| UME | Undergraduate Medical Education |
| GME | Graduate Medical Education |
| CME | Continuing Medical Education |
| CDC | Centers for Disease Control and Prevention |
| HPD | Health Providers professional development |
| TPD | Teachers’ Professional Development |
| NPS | Net Promoting Score |